By Lee Mulder, Chairman, Chapel Outreach Committee


Dr. Herbert Ainamani is in charge of the Chapel’s orphan rescue partners Juna Amagara Ministries in Uganda, E. Africa. He is also a PhD Clinical Psychologist who, with his colleagues at Mbarara University for Science and Technology, has prepared a paper for publication in scholarly journals in the U.S. and the U.K. exploring the mental hardship COVID-19 has had on the country and its people. The following is a summary of his report:
Since the inception of the COVID-19 virus in Wuhan China in December 2019, countries in Africa have prepared for dealing with the disease in a variety of ways. As of May 2, 2020, Uganda reported 85 confirmed cases, 52 recovered, and no deaths. It may be due to strict containment measures imposed by the government that has prevented the country with 45 million inhabitants from becoming another epicenter of deaths in the world.
On April 1, the government of Uganda put stringent preventative measures in place, including the closure of territorial borders, compulsory quarantine for all returnees from international travel closure of public and private transportation including commercial trucking and halting all non-essential services such as retail shops, restaurants, bars, and entertainment centers. All religious gatherings were forbidden; all educational institutions were closed. In order to
prevent pandemonium, a night curfew banning public gatherings was put in place. Campaigns for hand-washing with soap and the use of facial masks were launched.
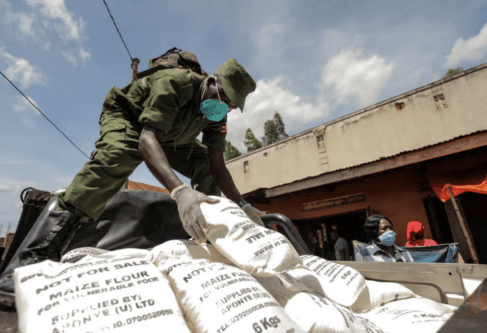
Many people, mostly urban dwellers, quickly ran short of food. It was illegal to travel to a grocery store; mass migration from urban towns where food was short to rural villages where subsistence farmers had food was blocked. Moreover, the homeless, the street children used to eating restaurant throwaways, and the very poor have been suffering since the restrictions were launched. Police actively “disperse” street children to places unknown and crime
increases as these children work to survive.
Security forces including the army police and Local Defense Units (LDUs) were mandated to enforce these Presidential directives, sometimes with excessive force. Many people, especially urban youth and women traders have been injured, humiliated, and arrested by security forces. Resentment by the citizenry has led to revenge and retaliatory violence against security personnel including throwing rocks at those trying to enforce the curfew. Incidence of violence is fueled by citizens witnessing scenes of aggression on social and mainstream media.

At the same time, communities are hunting down and shaming people believed to have been exposed to COVID-19. Once discovered, these people are picked up by health workers accompanied by armed personnel. Even people declared recovered from the virus are often stigmatized upon returning to their communities.
In a big disruption of African social culture, events like weddings, religious ceremonies, initiation ceremonies, and funerals have been banned or severely limited to small numbers. Travel restrictions have limited polygamous men from moving between their different homes. Self-isolation is a hard thing for Africans who are used to being among many people.
Another group facing trauma and stigmatization is the more than 20,000 international travelers who came into the country from or via countries heavily affected by COVID-19 at the onset of the pandemic. On arrival, they were placed in quarantine in government-chosen hotels and hostels in Entebbe town, some 45 minutes from the capital city. While there, the visitors were sequestered and required to pay for their food and lodging. The travel industry, a big part of the Ugandan economy has been shut down.
Taken altogether, the Coronavirus era, as we are calling it, is making a high impact on mental stability, greatly affecting the entire nation. By traumatizing children, we are most likely incubating psychological disorders affecting conduct, oppositional defiance, personality, substance abuse, prostitution, anxiety, and mood which will become permanent traits in poor individuals which will haunt our society for decades to come. Likewise, social distancing and
isolation in our society are already resulting in personal psychological disorders such as depression, anxiety, somatization, PTSD, and stigmatization. We will be studying and treating these disorders for many years to come.
Herbert E. Ainamani
Godfrey Z. Rukundo
Nolbert Gumusiriza
Mbarara University for Science and Technology
May 2020
Add Comment